
The majority of individuals with spinal cord injury experience significant symptoms related to neurogenic bowel dysfunction, e.g. 42% experience constipation and as many as 77% experience faecal incontinence.
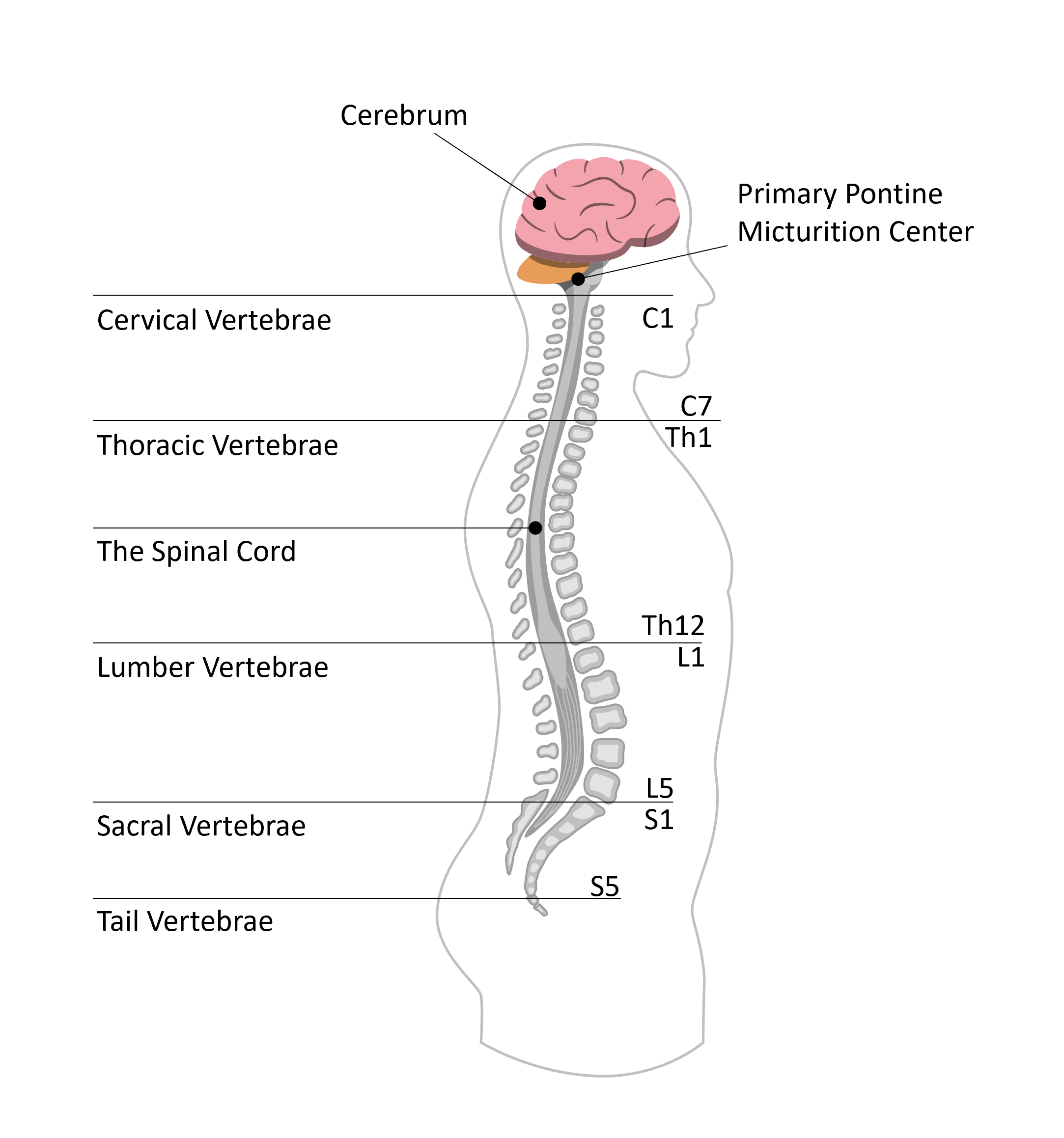
A spinal cord injury (SCI) can occur at any level of the spinal cord. It can either be a complete injury, with a total loss of sensation and muscle function, or incomplete, meaning some muscle control and feeling may remain. A SCI usually affects control over the bladder and bowel but depending on the level and completeness of the lesion, different symptoms occur. Three nerves are important for controlling the function of the bladder and bowel.
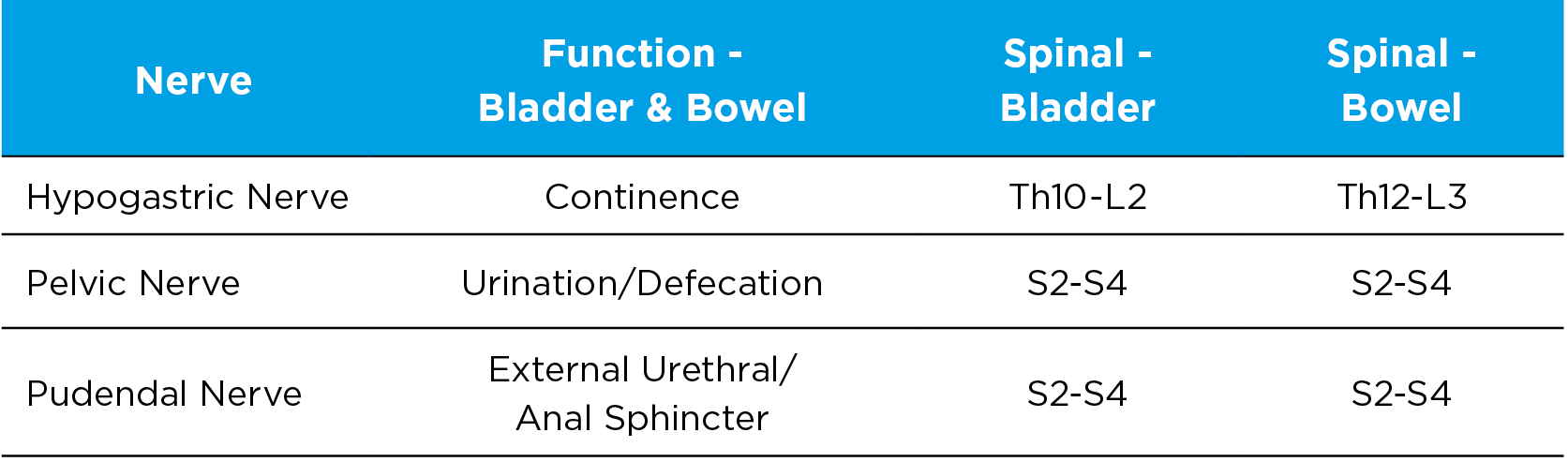
The nerves involved in bladder and bowel control are hypogastric, pelvic and pudendal nerve.
Bladder Problems
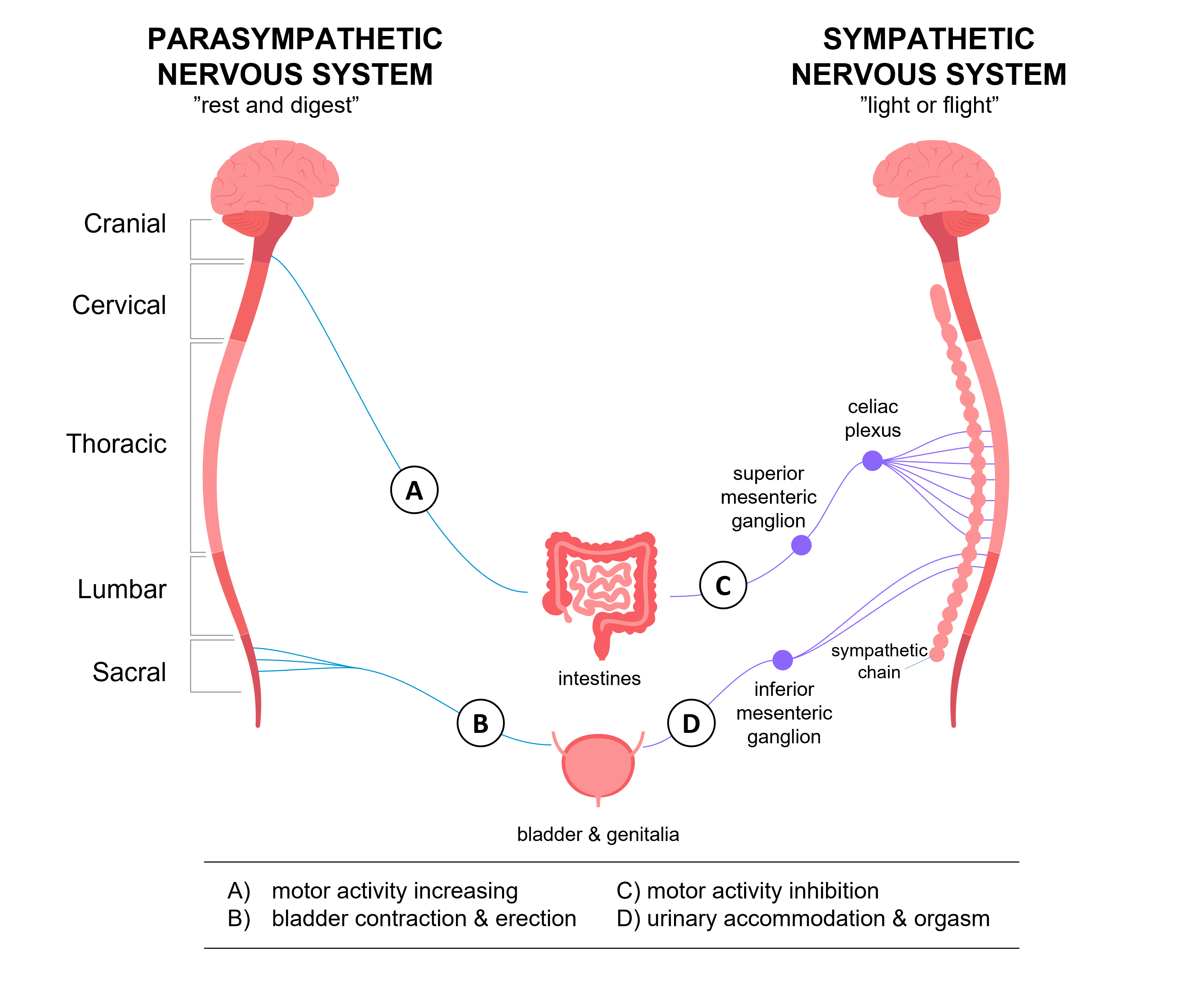
The body’s ability to store and empty urine is related to nerve and muscle function. When this is disturbed, the urine flow is affected and might cause a bladder dysfunction.
Overactive Bladder
Neurogenic overactive bladder from nerve damage is a common cause of bladder symptoms in SCI.
A SCI above T12 would typically result in a reflex, or spastic, bladder meaning involuntary control of the bladder. When the bladder fills above a certain level, a reflex will automatically trigger the bladder to empty, i.e. not knowing when the bladder will empty.
An overactive bladder may lead to storage symptoms, such as urinary urgency (a sudden urge to urinate which can be difficult to ignore or control), with or without urinary incontinence, increased daytime frequency and nocturia (night time voiding). Incontinence from urinary urgency is a common type of involuntary urinary leakage in both men and women with SCI.
Detrusor Sphincter Dyssynergia
Higher lesions can also lead to detrusor sphincter dyssynergia. A SCI can cause nerve damage and disruption of the nerve regulation of the micturition reflex. This can result in loss of control between the bladder detrusor and the external urethral sphincter muscle. Usually these two separate muscle structures act in coordination. Detrusor sphincter dyssynergia means the urethral sphincter muscle contracts instead of relaxes during voiding. This hinders the urine flow and causes the bladder pressure to rise, and this is a risk for backflow of urine from the bladder to the kidneys and urinary retention.
Underactive Bladder
A SCI below T12 would typically result in a non-reflex, or flaccid, bladder. This means that the feeling of a full bladder is lost and the bladder is at risk of being overfilled.
Underactive bladder is a condition where the bladder muscle (detrusor) is weak and cannot contract and/or storage capacity is less. This may lead to urine hesitancy and a poor or intermittent stream.
In general, people with underactive bladder have less sensation of when the bladder is full, and less capacity to contract the muscles involved in complete bladder emptying. Therefore, residual urine might be left inside the bladder, which can lead to urinary tract infection.
Bowel problems
People with SCI experience neurogenic bowel problems, which increase with age.
Higher lesions will result in slower colon transit times, up to double ‘normal healthy’ transit. This will lead to constipation and faecal retention/impaction.
A SCI above T12 would typically result in a reflex bowel with the following symptoms:
- Loss of sensation when bowel is full. The message between the bowel and the central nervous system (CNS) usually telling the bowel that it is full is not received
- Will continue to empty when stimulated
- A high rectal pressure
- The muscle controlling the opening and closing of the anus stays tight
- When the bowel gets full, it empties automatically, i.e. predisposed to inappropriate emptying
A SCI below T12 would typically result in a flaccid bowel, with the following symptoms:
- Loss of sensation when bowel is full
- Will not fully empty, even when stimulated. This is because the SCI has damaged the pathways from the bowel into the reflex center in the spine, i.e. there cannot be any reflex action
- The rectal pressure is low
- Predisposes to bowel soiling, i.e. faecal incontinence
The proximity of the bladder and bowel means that functional interaction is inevitable. It is therefore important to remember that some of the bladder and/or bowel symptoms may have a correlation, e.g. urinary leakage due to constipation.
Since there is such a close connection between the bladder and bowel, and problems arising in one area might also affect the other, it is important to remember to address them both to increase quality of life for the person affected.
The emotional and psychological impact of bowel problems with SCI can be devastating. Therapies should be aimed at understanding the physiological mechanisms, and tailoring treatments towards symptom management.